..by Terrance Hunsley
It is fair to say that there is no current model of health care delivery which is tailored to seniors. Despite being a significant portion of health care costs throughout Canada, seniors care is a part of a generic delivery model, with a few add-ons.
The existing model was built at a time when Canada had a much younger population. We needed to spread doctors across the landscape, and develop institutions – hospitals and residential institutions – placed to serve broad regions and populations. People could make appointments, jump into their cars, and go to get services. In emergencies, an ambulance could provide quick transportation across a broad region. Overall, Canadians were satisfied with their system. Most of the population were mobile and saw their doctor maybe a couple of times a year.
A few decades ago, Ontario and a few other provinces experimented with community health centres, which were intended to serve everyone in a geographic area. But they moved away from that and experimented with health teams led by doctors. Then they moved away from that, back to the old system. Now new doctors, paid on a fee-for-service basis, tend to set up in the suburbs, or in walk-in clinics where each symptom may require a separate visit because that’s how they make money.
But seniors have different health care needs
They are less mobile as they age, and driving a car is not always recommended. And they accumulate illnesses and chronic conditions, so they need monitoring, lab tests, changes in their meds. New conditions develop more often. Although they may have had a family physician to look after them over the years, chances are their physician is in the same age range, and is retiring.
Seniors are usually very attached to their neighbourhoods, where they may have moved to raise their families and form friendships many years ago. Yet when they get to be elder seniors and require continuing care and assistance with daily routines, they either have to hire expensive private care services, or move outside their community into a retirement home – if they are lucky enough to afford it. Many rely heavily on family and friends – most often daughters or other women, for unpaid care services.
What is the cost to the system for seniors?
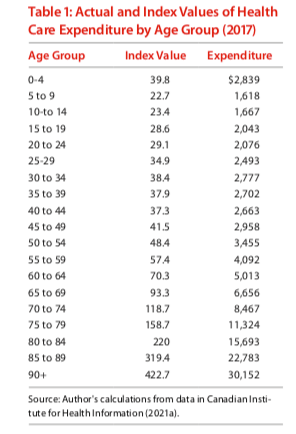
Let’s look at the amount of money spent from the health care budget for people at different life stages. The table below shows that babies and toddlers incur some significant costs to the system. After that, the usage of the system settles down nicely, until people get older. Then, the annual expenditure per senior goes up sharply, although the biggest portion is spent in the last six months of life.
With the numbers of seniors shooting up, the Fraser Institute projects that health care costs will increase rapidly.
Total health care expenditures for individuals aged 65 and older are projected to increase from $74.61 billion in 2019 to $110.04 billion in 2030 and then to $140.52 billion in 2040. This translates to an increase in health care expenditures for seniors of 47.5 percent from 2019 to 2030 and an increase of 88.3 percent from 2019 to 2040.
Total health care expenditures for individuals aged 65 and older are projected to increase from $74.61 billion in 2019 to $110.04 billion in 2030 and then to $140.52 billion in 2040. This translates to an increase
in health care expenditures for seniors of 47.5 percent from 2019 to 2030 and an increase of 88.3 percent from 2019 to 2040. These esti- mates assume that health care expenditures per capita remain constant at their 2017 values.
Even that projection assumes that people delivering care to seniors, people like personal support workers, and various levels of nursing care, will continue to be paid at existing wages. We know that some of those jobs are underpaid and exploit new immigrants and minority women.
Another study, done for the National Institute on Aging, projects that long term care costs will, in constant (inflation adjusted) dollars, triple over the next thirty years – also assuming current pay levels and a concomitant tripling of the informal care provided by friends and families.
So really, isn’t it time to design a care system for seniors? Putting it off, so popular among politicians, will be like watching the fuse burn on a time bomb.
What would help to provide better health service at lowest possible cost?
1. Focus on neighbourhoods. Serve people in clusters. Put health teams in place with geographic areas to serve. These could very well be expansions of current private practitioners facilities, or of hospital or university clinics. Expand community centres.
2. Set up nurse practitioner centres, for primary care and first-line gatekeepers. Link them to home care and assisted living, and to family physicians for more serious issues. Link them as well to remote monitoring and diagnostic technology and virtual visits. Link them to the informal caregivers.
3. If we want people to age in their homes and communities rather than high-cost residential and institutional facilities, we really have to improve the offer for home care services. Making people pay from their pocket for health care merely because they stay in their home and save the government money, seems unwise and unfair. Moreover, relying on families and friends to provide care could precipitate a crisis, since the age group that provides the most informal caregivers is not increasing at the rate of those who will require care. Medicare should cover health care, regardless of where it is delivered, and should be affordable to all.
4. Postpone long term residential care by providing assistance to community nonprofits to acquire property in the community and financing to develop housing options permitting people to live in smaller but accessible and flexible spaces with appropriate health support services. Encourage links to community centres for recreation, education, transportation. Take seniors care residences out of the hands of real estate developers, and let the value of property accrue to the community.
5. A progressive tax on wealth and high-value estates could be used to offset the extra costs. High-income households could also afford to pay a bit more.

You placed the getting old issues where I can understand.
LikeLike